|
jeudi 30 janvier 2014
Emphysematous Cholecystitis
|
| |||
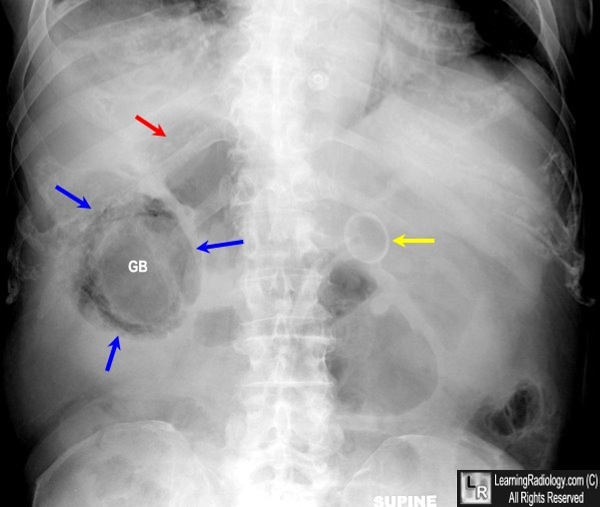 | |||
Emphysematous Cholecystitis. Supine view of the abdomen shows air in the wall (blue arrows) of the gallbladder (GB). There is also a lucency within the lumen of the gallbladder (GB) suggesting air inside the lumen. There is no air-fluid level visible because this radiograph is obtained supine with a vertical x-ray beam. Just superior to the gallbladder is another collection of air (red arrow) that represents a pericholecystic abscess. The yellow arrow points to the end of a PEG tube in the stomach.
|
Garland's triad (also known as the 1-2-3 sign or Pawnbrokers sign) is a lymph node enlargement pattern which has been described in sarcoidosis.
It comprises of:
- right paratracheal nodes
- right hilar nodes
- left hilar nodes
Involvement of right paratracheal nodes is not magical but rather reflects the ease with which these nodes are identified on plain radiography. Left paratracheal and aorto-pulmonary nodes are also frequently enlarged, but harder to identify 1.
mercredi 29 janvier 2014
The apple core sign, also known as a napkin ring sign, is most frequently associated with constriction of the lumen of the colon by a stenosing annular colorectal carcinoma.
Abdominal trauma, Shattered spleen, left renal segmental infarction and left hemothorax
CT bdomen with IV contrast revealed:-
- Hypodense zones are seen at upper pole of spleen.
-Hypodense area is seen at the left renal cortex.
-Hypodense lienorenal pouch.
-Laceated lower pole of spleen.
-Sparing the renal pelvic structures and vascular bed.
-all that mentioned above consistant with left side abdominal hematoma with splenic laceration ,,and related to grade III.
The haemosiderin cap sign refers to an MR imaging feature in some spinal tumourswhere a cap of T2 hypointense haemosiderin is above and / or below the tumour due to previous haemorrhage.
It is most often associated with spinal cord ependymomas, being seen in 20-33% of these cases 1. The sign however may also be seen in hemangioblastomas and paragangliomasand therefore it is suggestive of but not pathognomonic for ependymoma.
Inscription à :
Commentaires (Atom)